
By Blake J. Surina
Metabolic Equivalent of Task (MET)
In the late 1960’s to early 1970’s, the Pacific Northwest was a hotbed of pioneering research in exercise physiology. Dr. Robert Bruce at the University of Washington was already being touted as the “Father of Exercise Cardiologyâ€. Publishing his original research in 19631the Bruce treadmill testing protocol for identifying latent heart disease became the standard in the United States by the 1970’s. Included in his long list of accomplishments was the introduction of the concept of Metabolic Equivalent of Task or MET.

A landmark study done by Passmore and Durnin2in 1955 sought to collect the metabolic work costs associated with hundreds of physical activities and labor tasks. The research quantified these physical activities in averagecalorie cost per minute, thereby introducing the possibility of data that would not represent larger and smaller subjects accurately.
Bruno Balke3, while employed at the School of Aviation Medicine in San Antionio, published research in 1954 that created a treadmill protocol to estimate a subject’s maximal aerobic power. Using a speed of 3 mph, Balke increased the elevation 2.5% every couple of minutes. He discovered that an elevation change of 2.5% during exercise, increased the metabolic rate approximately one multiple of the subject’s resting metabolic rate. This served to minimize the effect of variations in body dimensions when predicting exercise metabolism, thus providing a method to measure metabolic work based on multiples of resting metabolic rate.
Dr. Robert Bruce was able to provide multiples of a subject’s resting metabolic rate associated with the exercise stages of his Bruce Treadmill Protocol. These multiples of resting metabolic rate he termed Metabolic Equivalent of Task, or MET’s. This provided a way to prescribe exercise and predict oxygen consumption relative to the subject individual body dimension. Theoretically, he felt that all subject’s performing a set amount of work on a treadmill would record the same MET level for their effort.
As early as 1952, Dr. Robert Bruce partnered with the bioengineer Wayne Quinton in designing the first treadmills for widespread use for Medical Exercise Testing.   With the widespread use of the Bruce protocol, the leading cause of death being heart disease, and the sudden popularity of the home treadmill, (following the release of the book “Aerobics†by Dr. Ken Cooper in 1968), cardiac rehabilitation was in its infancy.  In 1971, Dr. Bruce began the Seattle Heart Watch Program focused early diagnosis and treatment of heart disease.Â
One of the early advocates of the Seattle Heart Watch Program was Dr. Howard Pyfer, who created the Bellevue CAPRI program providing cardiac rehabilitation services to the Northwest.  The Seattle based CAPRI program was recognizedÂ

as the third cardiac rehabilitation program in the country.  Ozzie Khartoon was hired to direct the new CAPRI program, and to develop progressive exercise levels for heart patients using METs as a unit of work intensity.                               Â
To do this original work, Western Washington University was selected because of the recent acquisition of the new Beckman MMC metabolic cart in 1976. Beckman in 1975-1976 marketed the first portable Metabolic Measurement Cart (MMC). The MMC had the ability to record the oxygen consumption measurements and the newly created MET value of the work being performed a real time. Using a an early Quinton Treadmill and the Beckman MMC cart, determination of the work levels for CAPRI was completed by Blake Surina and Mark Mitsui in 1980.
Beckman MMC Cart (1976)

Quinton treadmills in the late 1970’s used controllers that were analog, with speed and elevation controls only. By the 1980’s Quinton integrated computerized controllers for medical treadmills used in exercise testing. This allowed treadmill protocols to be programmed, by the testing technician, into the treadmills controller. VO2 (in ml/kg*min-1) and MET values could now be displayed in real time while exercising. Wayne Quinton programmed the Bruce Protocol as the default protocol in the 645 controllers for the Quinton Q55 and Q65 treadmill manufactured the early 1980’s.
Quinton Analogue Controller (1979)
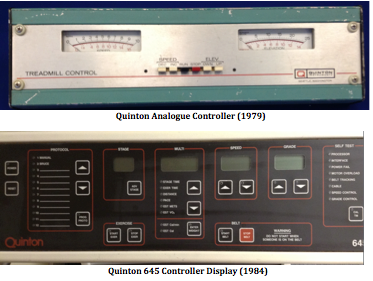
Quinton 645 Controller Display (1984)
Dr David Parker, recently appointed the chief physiologist for the Boeing Company in 1977, and was a true pioneer of the Corporate Employee Wellness Program in the United States. Dr Parker’s lab at this time was using the Ergopneumo-test Metabolimeter  (Jaeger – Germany), a very large a cumbersome metabolic computer and the newest Quik-Prep system developed by Quinton Instruments to prepare a patients EKG electrodes before exercise testing.  Dr. Parker was a early contributor of the Seattle Heart Watch Program, and reported a cost to Boeing of over 100,000 dollars to replace a Boeing executive that would be lost as a victim of a heart disease.                                                                                                                  Â
Compensated MET (cMET)
In 1977, Per-Olof Astrand published his 2ndedition of “Textbook of Work Physiology†showed a graph by Vaage and Hermansen.  The graph showed elite Norwegian athletes oxygen uptakes plotted by weight in absolute values (l/min), relative values (ml/kg*min-1) and by mass (ml/kg(-2/3)*min-1).   This was the first data to demonstrate allometric scaling of oxygen consumption for athletes, but carried no citation for any published research.  It was apparent from the graph that smaller athletes were more metabolically active than larger athletes on a per weight basis.  Using the -2/3 exponential relationship to mass, a way of directly comparing individual performances in lieu of differing body dimensions was created.
In the early to mid 1980’s Exercise Physiologist Blake J. Surina, developed and later patented the Compensated METor cMETfor body dimension scaling. To compensate for the body dimensions, Surina created a correction factor so existing units commonly used to measure oxygen consumption, i.e. METs, or ml/kg*min-1could still be used.
There continues to be disagreement between researchers as to what the scaling exponential ratio to the subject’s mass should be. Seymore and White4 of England defended the use of the -2/3, and Geoffrey West of Stanford University5the -3/4. Most agree it is somewhere in this range. Surina found that in maximal physical efforts the -2/3 exponential relationship to mass gave better results, and that the -3/4 was better for resting metabolism. Surina’s patented range included the range of exponents from .63 to .75.
By adjusting metabolic variables down from the 1:1 relationship of the Bruce linear model, to the allometrically scaled -2/3 exponential relationship involves a correction of 1/3. This can be done with the creation of a simple correction factor.
                       Individuals Weight ^(1/3)
Ref. Population Weight ^(1/3)Â Â Â Â =Â Â Â Correction Factor
In the simplest terms, the cube root of the individuals weight over the cube root of the reference population weight equals the correction factor. This correction factor is multiplied by the MET score and becomes the individual’s allometrically scaled equivalent, a Compensated METvalue, or cMET. What started out nearly 50 years ago, the ability to evaluate and prescribe workloads independent of a subject’s body dimensions, is now a reality.